Use of High Velocity Therapy for Reversing Pneumothorax: a Case Report
By Marcos Cesar Ramos Mello, Hospital BP – A Beneficência Portuguesa de SP, Luciana Dalla Torres, Hospital BP – A Beneficência Portuguesa de SP, Alessandra Cristina Marques dos Santos, Hospital BP – A Beneficência Portuguesa de SP, Heloisa Maria Khader, Hospital BP – A Beneficência Portuguesa de SP, Juliana Pacheco, Hospital BP – A Beneficência Portuguesa de SP.
Vapotherm’s high velocity therapy is a tool for treating respiratory distress. Although individual results may vary, Vapotherm believes this case study is an example of the clinical benefit Vapotherm’s high velocity therapy can have in an ICU setting. Practitioners should refer to the full indications for use and operating instructions of any products referenced herein before prescribing them.
Introduction
Pneumothorax, or the presence of air in the pleural cavity, is a frequent condition in clinical practice. The standards of conduct for the pneumothorax approach depends on the patient’s clinical conditions and the magnitude of pneumothorax. When high velocity therapy is used, fresh gas quickly occupies the nasal cavity and pharynx, eliminating gas rich in CO2 from nasopharynx dead space through the ‘open’ system. (Figure A)
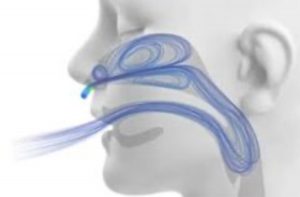
Thus it is believed that there is an increase in the absorption speed of pneumothorax, by decreasing the alveolar pressure of nitrogen, which passively forces the absorption of air from the pleural cavity to the alveoli.
Objective
The objective of this study was to describe the initial experience in the use of high velocity therapy as an alternative support in pneumothorax reversal.
Case Report
We report the case of a 2- month-old patient weighing 5.0 kg, height 55 cm, male, who underwent total correction surgery of Tetralogy of Fallot with monocucuspid number 8, arterial canal ligation and enlargement of the left pulmonary artery. He was admitted to the ICU from the operating room, without complications in the surgical procedure, cpb time 155 minutes, receiving Adrenaline 0.1 Primacor 0.5, with sedation. Physical examination: Regular general state, hypocolored, in mechanical ventilation, no fever. Pulmonary auscultation without adventitious noise.
He was extubated in the 1st Postoperative period without complications, installed mask oxygen therapy with 5L/min without signs of respiratory distress, suspended adrenaline and released diet. Physical examination: HR 162 O2 saturation of 95% BP 70/42 (52) hypocolored, hydrated, afebrile, flat abdomen, flaccid, full and symmetrical pulses.

Patient in the 2nd Postoperative period, after removal of right pleural drain, a simple chest x-ray was performed that showed moderate pneumothorax on the right (Figure B), patient remaining without signs of hemodynamic instability, we chose to initiate high velocity therapy, with the Precision Flow device (Vapotherm Inc., Exeter, New Hampshire, United States), and the following initial parameters, FiO2 of 100%, Flow of 10L/min and temperature of 36°C were adjusted. Physical examination: Patient follows hypocolored, hydrated, afebrile, active and reactive, pulmonary auscultation with decreased bilateral sounds + to the right, flat abdomen, flaccid, full and symmetrical pulses.
After 18 hours of the beginning of high velocity therapy, a new plain chest x-ray is performed that showed the total resolution of pneumothorax (Figure C). Started weaning of high velocity therapy, child with no signs of respiratory distress, 95% O2 saturation suspends high velocity therapy.

Results
In the case reported here, the patient benefited from the use of high velocity therapy, since pneumothorax resolution was obtained in addition to the improvement of pulmonary auscultation in less than 24 hours after the start of treatment, remaining with good respiratory pattern, hemodynamically stable and with good tolerability of the therapy, especially when it comes to a patient in the postoperative period of congenital heart disease surgery.
Conclusion
The use of high velocity therapy appeared to be effective, safe and presented good tolerance for the patient, suggesting that it is a possible adjuvant in the management of treatment for pneumothorax reversal.